











Retained primitive reflexes can keep a child from reaching their full potential. Primitive reflex integration done with daily exercises can improve core autism symptoms. Therefore, if your child has social-emotional, academic, sensory, behavioral, or motor skills challenges, primitive reflexes are worth investigating.
This article will cover:
- What are primitive reflexes
- Why primitive reflexes are important
- Reasons for retained primitive reflexes
- Testing for retained primitive reflexes
- List of Primitive Reflexes
What are Primitive Reflexes?
Primitive reflexes are automatic, involuntary movements present at birth that protect and help an infant to survive outside the womb. As such, they are called “primitive” because they are an early brain function and support the brain’s continued maturation and development.
Why Primitive Reflexes are Important
Early primitive reflex movements pave the patterns of neural networks and myelination of brain pathways. These allow connections between various areas of the brain important for learning, behavior, communication, and social emotional skills.
Like steps of a ladder, each primitive reflex helps to develop the sequential pathways and connections needed for the next step in the ladder of development. Therefore, as movement patterns are repeated, new neural pathways are sequentially developed in the brain.
During the first year of life, each involuntary primitive reflex response gives way to a more voluntary movement (postural reflex). This reflex integration is part of the maturing of the central nervous system (CNS). In addition, the presence and strength of primitive reflexes in infancy can be a helpful indicator of nervous system development. If a primitive reflex remains active causing a child to skip a step in the developmental ladder, this is referred to as a “retained primitive reflex.”
When primitive reflexes are retained, they impair the maturation of voluntary, postural reflexes that contribute to higher development and learning. Consequently, this puts a child at more risk for challenges with social emotional, academic, sensory, behavioral, and motor skills.
Reasons for retained primitive reflexes
Primitive reflexes may be retained for a variety of reasons. In addition, they may become active again in children or adults.
- Trauma, illness, or shock during pregnancy.
- Premature, traumatic, caesarean or lengthy delivery.
- Extended time in car seats, carriers, walkers, jumpers.
- Illness, injury, chronic stress, trauma.
- According to a Clinical Methods text listed by the National Institutes of Health, the rooting and palmer retained reflexes are associated with frontal lobe disorders and certain forms of neurologic disease.
Testing and Integrating Retained Primitive Reflexes
It is helpful to test a child for retained primitive reflexes to see if their nervous system is operating in an immature and protective/defensive state. After testing for retained reflexes, a skilled practitioner can compile a movement program to help integrate reflexes.
However, you can integrate these primitive reflexes without a program or investing any money at all. But, you do need to invest the time. Integrating retained primitive reflexes requires doing daily exercises specifically designed to properly integrate the reflex. For example, exercises need to be done at least once or twice daily over months in order to retrain the body, and for the brain to form new pathways. Videos are included under each reflex with examples of the exercise.

Practitioners that Address Primitive Reflex Integration
There are several types of practitioners that address primitive reflex integration. It is a specialty area that requires formal training. These individuals are often chiropractors, or specially trained occupational or physical therapists.
In addition, Brain Balance, MNRI, or Neurodevelopmental Movement are methodologies that include and emphasize primitive reflex integration. Each approach has a directory of trained practitioners available on their website to enable you to locate someone near you.
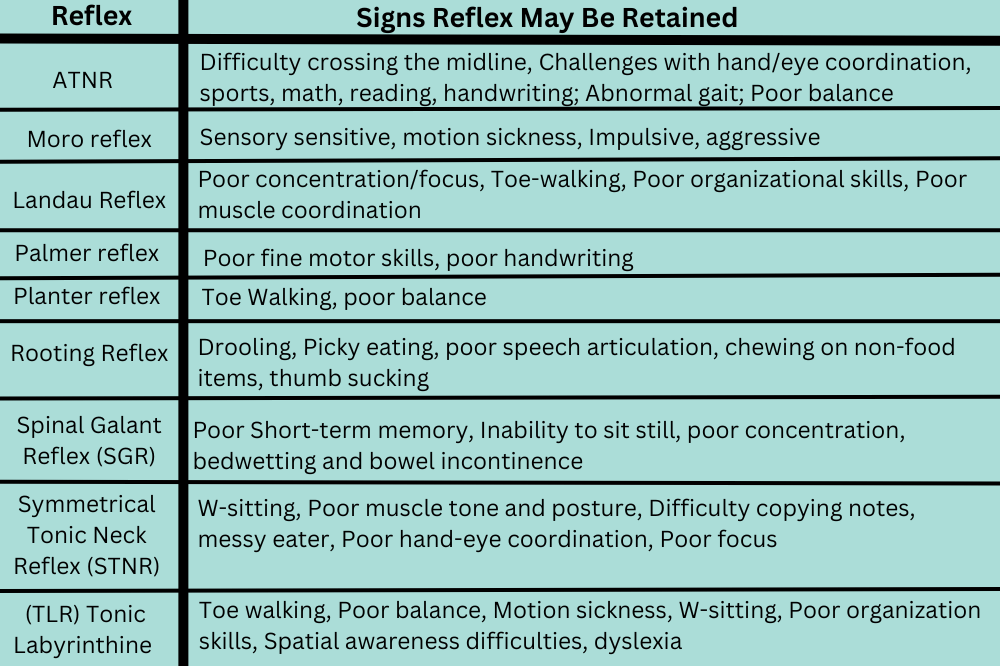
List of Primitive Reflexes

Palmer Reflex
When babies wrap their fingers around someone’s finger towards their palm, they are demonstrating the palmer grasp reflex. Since babies are unable to organize movements to voluntarily grab things initially, the palmer grasp reflex helps set the foundation for that voluntary ability to develop. As children develop, the palmer reflex gives way to the child learning to use their pincer grip verses just their palm and fingers for a strong grasp.
Observing the palmer grasp:
When your newborn grasps your finger, you experience the palmer grasp. The response to stimuli on the palm includes two phases: finger closure and clinging.
Usually integrates by 5 to 6 months of age.
Symptoms of retained palmer grasp:
- A weak grasp
- Poor fine motor skills
- Poor handwriting
Video with exercise:
Exercise to strengthen the pincer grip and palmer reflex: How to help the Palmar primitive reflex- Pincer grip rubber bands – YouTube

Planter Reflex
The Babinksi/Plantar Reflex helps to coordinate the muscle patterns in our lower body to help us feel grounded, secure and stable.
Observing the Babinksi/Plantar Reflex:
The Babinski reflex is seen in early development when we stroke the sole of the foot and the toes extend up and out. This response should integrate into the plantar reflex by one to two years of age.
The Plantar reflex is the integrated form of the Babinski reflex. In healthy development after age two, the stroke on the sole of the foot should cause the toes to flex downward or curl in. However, if the toes still extend up and out after age two, this is called a ‘retained Babinski reflex.’
Identifying characteristics of a retained Babinski/Planter reflex:
- Toe Walking
- Issues with proprioceptive and vestibular systems
- Muscles in the back of the legs are affected, altering gait
- Trouble with balance Gravitational insecurity
- Trouble with vestibular, visual, and sensory systems
Video with exercise:
Testing and integrating Babinski/Plantar Reflex: Babinski Reflex: Brushing Integration – YouTube
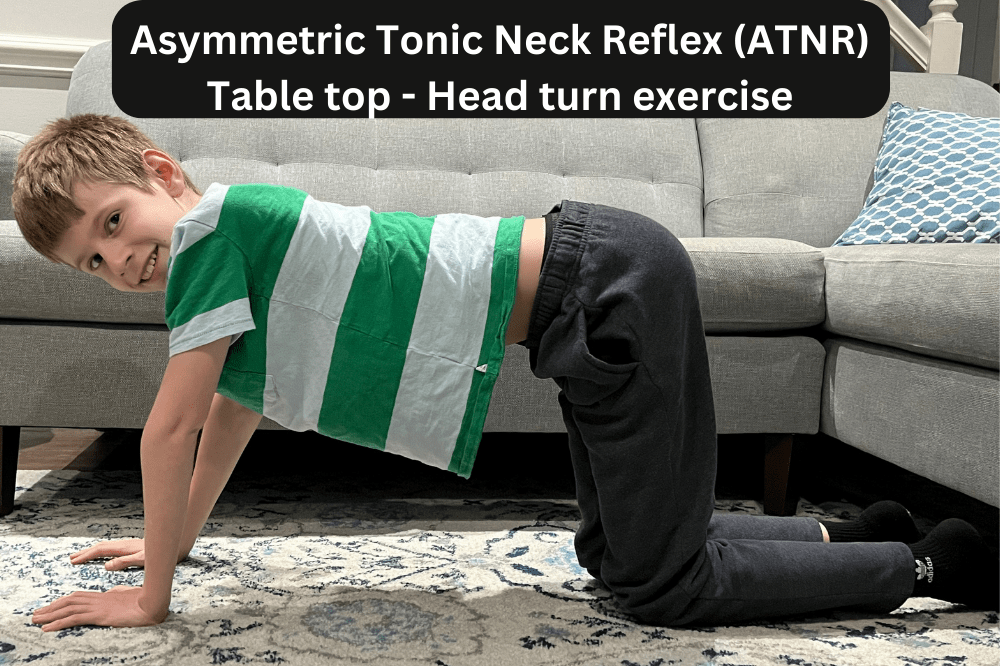
Asymmetric Tonic Neck Reflex (ATNR):
ATNR is sometimes called the “fencer’s pose”. It is an important reflex in the development of one-sided movement, hand eye coordination and muscle tone.
Observing ATNR:
When a baby is lying down on their back, the head turns to one side and the arm and the leg on the same side will extend. Simultaneously, the arm and the leg on the opposite side will flex.
Onset in utero and usually integrates by 5-7 months
Symptoms common with Retained ATNR:
- Difficulty with activities that require crossing the midline of the body
- Immature handwriting
- Eye, ear, foot, hand dominance may not all be on one side
- Abnormal gait
- Challenges with hand/eye coordination, sports, math, reading
- Poor balance or depth perception
- Studies in 2004 and 2007 indicated that retained ATNR can impact reading development.
- *Symptoms are not diagnostic.
Videos with exercise:
- Provides an overview of assessing ATNR: Testing for a persistent ATNR (Asymmetric Tonic Neck Reflex) using Schilders and Quadruped Testing – YouTube
- Provides a quick assessment of ATNR and suggested exercises to help integrate: How to assess and treat a retained ATNR – YouTube
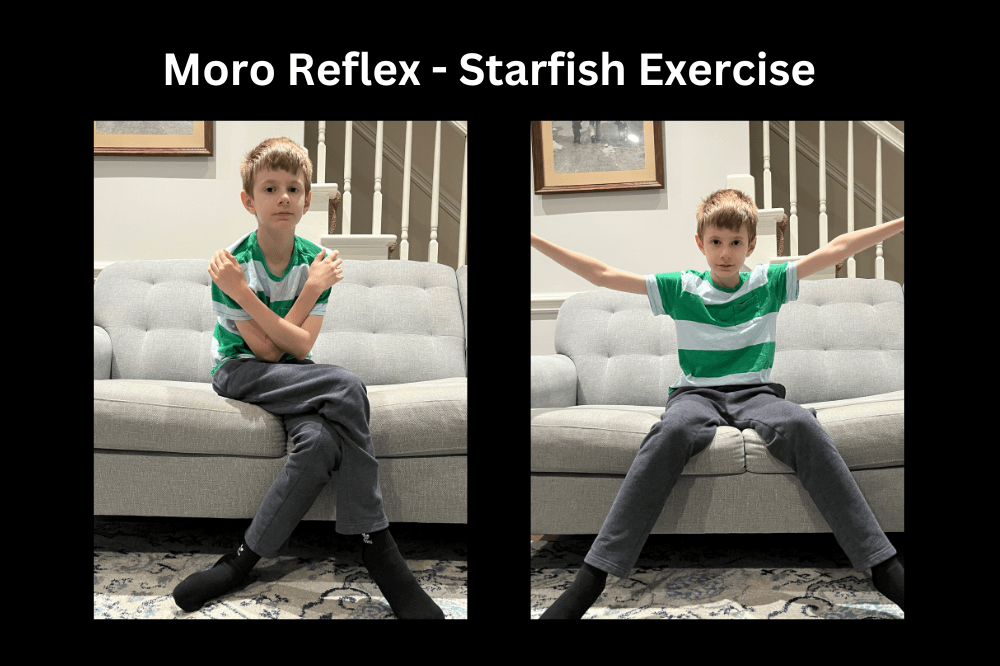
Moro Reflex
The Moro reflex is also known as the “startle” reflex. This is a survival response that provides an infant with an instant arousal in response to stimuli. This enables the child to sense and fear danger as a mechanism to protect themselves.
Observing the moro reflex:
When an infant is stimulated by a loud noise or feel their head drop, their reflex response is to extend their arms and legs suddenly and then draw them back inwards towards their body. In addition, a retained moro reflex can sometimes be the result of caesarean section, traumatic or prolonged births.
Usually integrates by 5-6 months of age.
Symptoms common with retained moro reflex:
- Hypersensitive / reactive or under sensitive/reactive to sensory stimuli such as light/sound/touch.
- Oversensitive to motion causing car sickness.
- Impulsive/aggressive/overreacts.
- Emotional immaturity.
- *Symptoms are not diagnostic.
Videos with exercise:
- Testing for retained moro reflex: Testing for a Persistent MORO reflex (Moro Test, Crossover Balancing, Pigeon/Duck Walk) – YouTube
- Starfish exercise laying down for retained moro reflex: Moro Exercise: The Starfish – YouTube
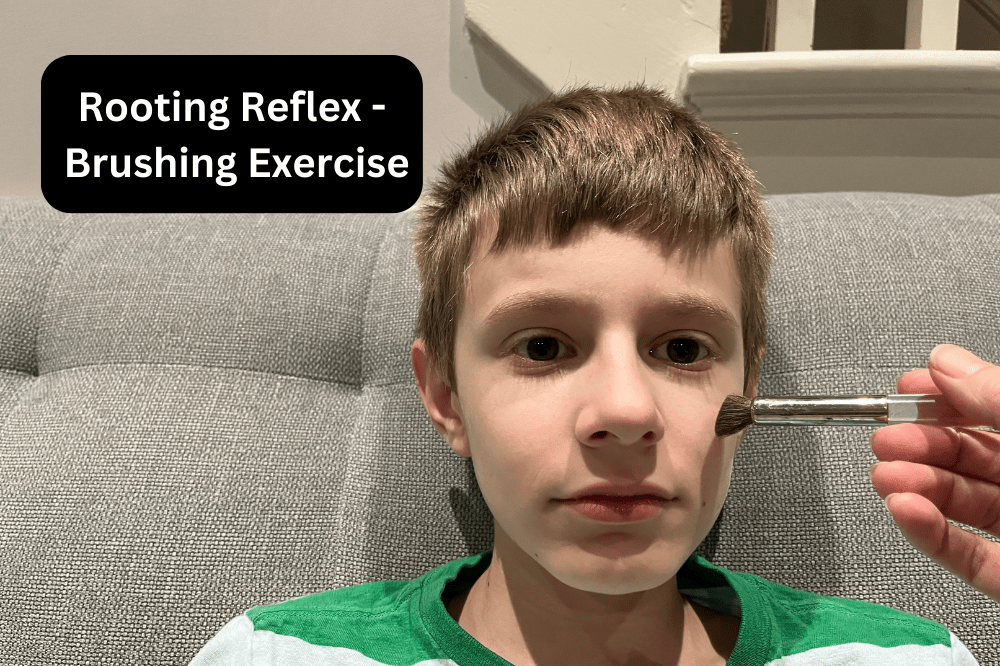
Rooting Reflex
The rooting reflex enables a newborn to turn towards the breast or bottle to feed.
Observing the rooting reflex:
When an infant’s cheek is lightly touched, look for mouth opening, or a turn toward the stimulation.
Usually integrates by 4-6 months of age.
Identifying characteristics that may indicate a retained rooting reflex:
- Drooling
- Picky eating
- Speech articulation
- Resistance to textures of some foods
- Constant chewing on clothes or toys
- Thumb sucking past the normal age
Video with exercise:
- Testing and addressing retained rooting reflex: Rooting Reflex: Brushing Integration – YouTube
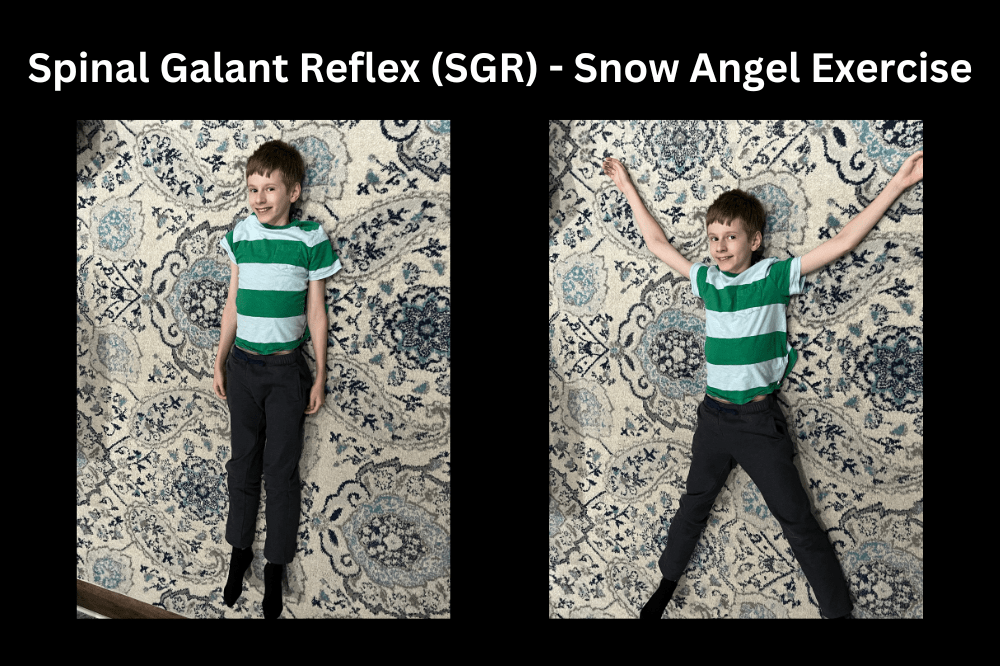
Spinal Galant Reflex (SGR)
The spinal galant reflex is critical for the baby as their body cooperates with the mother’s body in the progression down the birth canal and is important in the development of the vestibular system. Therefore, it encourages movement and development of range of motion in the hips and in preparing a child for crawling and walking.
It is present at birth and should be fully integrated by 3 to 9 months old.
Symptoms of retained spinal galant may include:
- Poor Short-term memory
- Inability to sit still (particularly in the region of the hips).
- It is known as the ‘falling out of the chair” reflex
- Poor Concentration
- Bedwetting, and bowel incontinence beyond the age of 5.
- Intolerance of food textures and waistbands.
- It can contribute to scoliosis when one side is more activated or back pain in older children and adults.
Video with exercise:
- Snow Angel exercise to help integrate retained spinal galant: Snow Angel Exercise – YouTube
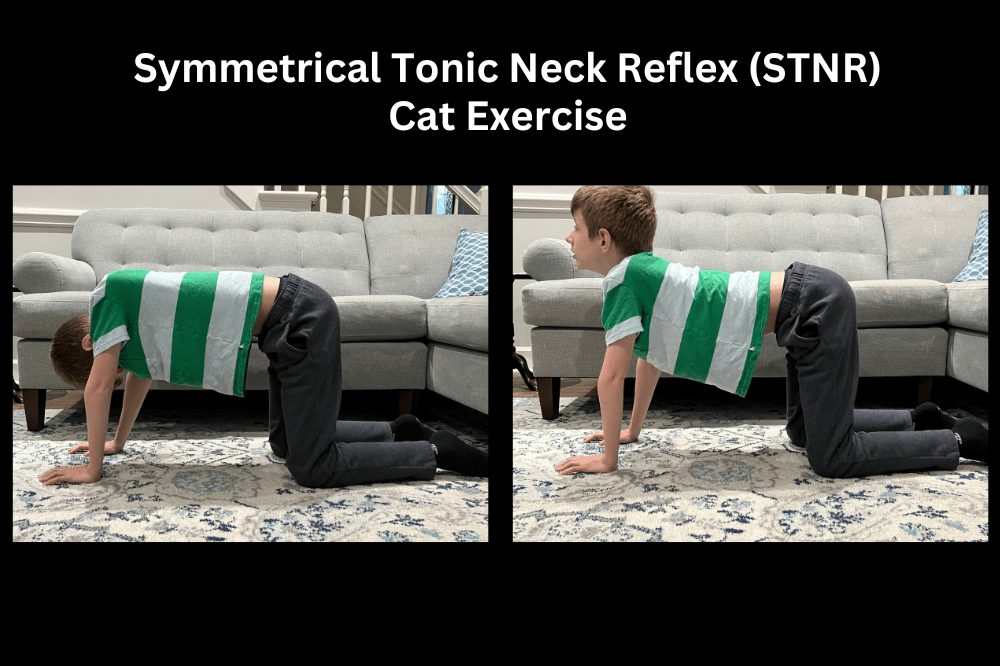
Symmetrical Tonic Neck Reflex (STNR)
STNR helps an infant develop the ability to be on all fours in preparation for crawling. This reflex helps to develop the ability to use the upper body and lower body independent of one another which is critical for posture, hand-eye coordination and focus.
Observing STNR:
Lying on their back, an infant will likely assume the “fencing position.” The head turns with the arm and leg of one side extended and the other arm and leg flexed. Another consideration is if lying on the back, the head tilts up towards the navel, legs will contract at the knee. When the head lays back down, the legs straighten back out.
Onset at birth and then subsides. Emerges again around 6-9 months (to assist with crawling) and usually integrates by 9-12 months of age.
*As STNR appears, ATNR should go away.
Common symptoms of retained STNR:
- “Bear Walking” on hands and feet instead of crawling on hands and knees.
- Scooting while sitting.
- Skipping the crawling stage and going directly to walking.
- Preferring to lie on the floor instead of sitting and/or sitting in the “W” position.
- Difficulty copying from the classroom board.
- Vision accommodation and tracking difficulties.
- Messy eater.
- Challenges with reading and learning to swim.
- Low muscle tone and poor posture.
Video with exercise:
- Quick assessment of STNR and suggested exercise to help integrate: How to assess and treat a retained STNR – YouTube
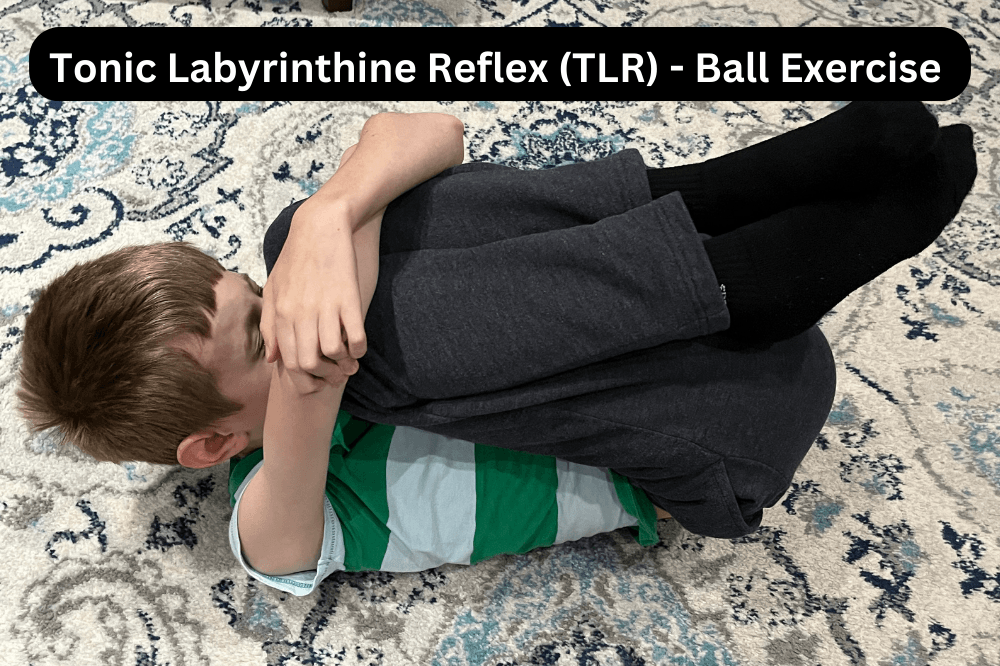
Tonic Labyrinthine Reflex (TLR)
Observing the TLR
There are two phases of the TLR. Firstly, this reflex is present in utero as the fetus’ head is forward of the spine and the limbs are pulled into the “fetal position.” During the birth process, TLR helps the fetus extend down and out of the birth canal. Secondly, post birth, this reflex is best seen during tummy time when the infant is extending their head, neck and limbs in a superman position. The reflex helps the infant open up the spine from the curved spinal shape in utero.
Usually integrates by 4 months of age.
A retained TLP impacts the way the head sits on the spine. In turn, this impacts the way a child navigates their body in the space around them, with gravity, and in feeling grounded with their steps. Consequently, these challenges can contribute to both balance and muscle tone issues.
While not diagnostic symptoms, these are some of the common features with retained TLR:
- Poor posture
- W-sitting
- Weak muscles
- Decreased balance
- Poor eye motor skills
- Visual perceptual challenges
- Auditory processing difficulties
- Poor organization skills
- Poor sense of space and time
- Poor sequencing ability
- Spatial awareness difficulties
- Dyslexia, dyscalculia and/or dysgraphia
Videos with exercise:

Landau Reflex
The Landau reflex is not present at birth, therefore it is not a primitive reflex. It is a reflex that helps other reflexes integrate.
It is developed around 4 months of age as the child begins to extend their legs so they are raised while the head and chest lift up.
Usually integrates by age one.
Signs of retained landau reflex include:
- Poor concentration
- Poor focus
- Tension in back of legs
- Toe-walking
- Poor organizational skills
- Poor muscle coordination between upper body and lower body.
Video with exercise:
- Exercise to integrate Landeau Reflex: Primitive Reflex Landau Reflex Superman
Conclusion
As you can see, primitive reflex integration is an important part of child development and it can be done at any time in a person’s life. Furthermore, we can see improvements in many areas including socialization, behavioral, and both gross and fine motor capabilities once the primitive reflexes are integrated.
Additional Video:
Comprehensive Video of Fear Paralysis/Moro, TLR, STNR, ATNR and Spinal Galant retained reflexes:
Additional Reading:
Assessment of Primitive Reflexes in High-risk Newborns (nih.gov)